

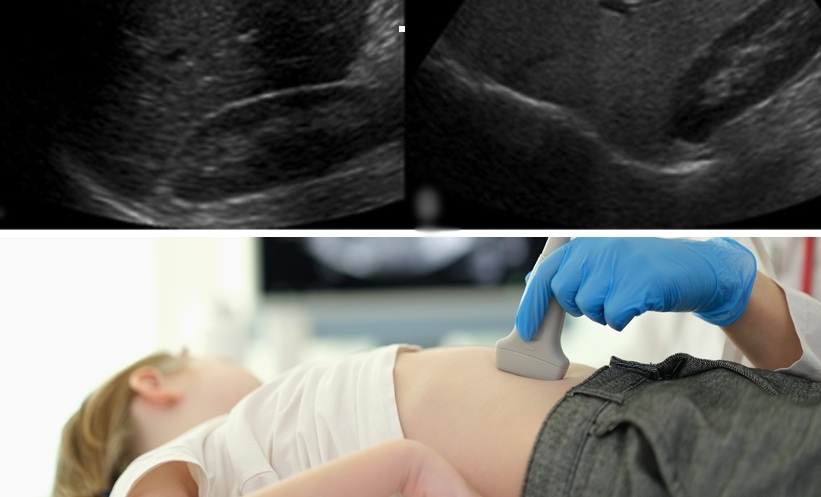
Paediatric liver disorders are fast becoming a serious public health crisis in India, fuelled by both infectious agents and lifestyle-related triggers. Hepatitis in children—primarily linked to viruses like Hepatitis A and E—continues to spread due to persistent malnutrition, poor sanitation, and delayed diagnoses. Despite progress in Hepatitis B immunization, glaring gaps remain. Hygiene education, robust healthcare infrastructure, and grassroots-level awareness—especially in rural and underserved areas—remain woefully inadequate.
Compounding the challenge, the recent global rise in unexplained acute hepatitis cases among children has heightened the urgency. India must now strengthen its surveillance systems, upgrade diagnostic facilities, and implement early intervention protocols. Without swift action, children face the grave risk of liver failure and other life-threatening complications.
In parallel, paediatric fatty liver disease is silently surging. The culprits: excessive intake of calorie-rich, nutrient-poor foods, increasingly sedentary lifestyles, and mounting urban stress. These factors are driving a rapid increase in non-alcoholic fatty liver disease (NAFLD), even among children with a normal body mass index. Although genetics play a role, diet remains the most significant—and modifiable—risk factor.
The solution lies not in blame, but in collective empowerment. We need widespread nutritional education, stricter regulation of food marketing aimed at children, mandatory physical activity in schools, and the overhaul of mid-day meal programs. A coordinated, multi-sectoral strategy must promote healthier daily choices and build long-term resilience in our youth.
At the Illness to Wellness Awareness Conference on Prevention, Diagnosis, and Treatment for Hepatitis, hosted by the Illness to Wellness Foundation, Dr. Sakshi Karkra, Head of Paediatric Gastroenterology & Hepatology at Artemis Hospital, shared critical insights in an exclusive conversation with The Interview World. She demystified paediatric hepatitis, outlined the national landscape of this growing concern, recommended concrete steps to prevent and manage fatty liver disease, and emphasized the critical role schools play in shaping children’s food choices. She also highlighted essential medical protocols to address mother-to-child transmission of hepatitis during childbirth.
Here are the key takeaways from her enlightening conversation.
Q: Could you explain what paediatric hepatitis is and provide an overview of the current situation regarding this condition in the country?
A: At present, hepatitis infections among children are clearly on the rise. This trend becomes even more alarming when we consider the parallel surge in paediatric fatty liver disease. Cases are escalating rapidly.
A significant number of children are becoming overweight—not due to medical conditions, but because of unhealthy lifestyles. Physical activity is nearly absent. Most children spend long hours glued to screens while consuming excessive amounts of junk food. The impact is stark. Around 10–20% of children who visit our outpatient department (OPD) for unrelated issues are also diagnosed with fatty liver—often incidentally. That’s deeply concerning.
Yes, vaccine-preventable forms of hepatitis can be controlled through proper immunization and early screening. But today, we face a far more complex challenge, particularly in urban and millennial populations. In these cities, the real epidemic brewing is fatty liver disease among children.
Combating paediatric fatty liver must become our top priority. Without urgent intervention, it is poised to become the dominant paediatric liver issue in the coming years.
Q: What steps do you recommend individuals take to manage or reverse fatty liver disease effectively?
A: Guidelines for adults differ significantly from those for children—mainly because the causes of liver disorders in adults often include infections, alcohol consumption, and high-stress lifestyles. In contrast, paediatric liver disease stems almost exclusively from poor dietary habits and lack of physical activity.
This makes prevention in children both simpler and more urgent.
As parents, we have a critical responsibility to instill healthy habits early. It starts with what we feed our children. A simple rule applies: if it comes in a packet, avoid it. Packaged and processed foods—regardless of branding—are rarely beneficial. Instead, focus on what comes from nature: fresh fruits, green vegetables, and wholesome home-cooked meals.
Eating out occasionally is acceptable, but it must remain the exception—not the routine. Equally important, we must eliminate bottled drinks from our children’s diets altogether. These beverages—whether sugary sodas or so-called “diet” alternatives—pose serious health risks. Even diet sodas can disrupt the brain’s satiety signals, causing increased hunger and encouraging overeating. The illusion of “zero calories” masks a deeper metabolic imbalance.
Natural, unprocessed foods should form the foundation of every child’s diet.
However, nutrition alone isn’t enough. Screen time must also be strictly regulated. Ideally, limit it to no more than one hour a day, including television, computers, and smartphones—unless it’s required for exams or homework. Simultaneously, ensure children engage in at least one to two hours of physical activity daily.
These changes are non-negotiable if we hope to protect the next generation from lifestyle-related liver diseases. The path forward is clear: less screen, more green—both on their plates and in their routines.
Q: In your view, what is the evolving role of educational institutions in addressing the broader developmental needs of students beyond academics?
A: Schools play a pivotal role in shaping children’s health, both through nutrition and physical education. In cities like Gurgaon, many schools now offer in-house lunch programs. While these initiatives aim to promote healthy eating, the reality often falls short.
When parents share their children’s school menus with me, I frequently see fast food items—burgers, fries, and similar ultra-processed meals—making regular appearances. These should not be part of a child’s daily diet. Schools must eliminate such foods from their menus and replace them with balanced, nutritious options that support physical and cognitive development.
Moreover, health education must become an integral part of the school curriculum. Children need to learn—consistently and early—about the importance of healthy eating, the dangers of poor lifestyle choices, and the lifelong benefits of regular exercise.
Equally critical is the role of physical education. Unfortunately, most students report having PE sessions only once or twice a week. That’s simply not enough. Physical activity should be a daily, non-negotiable part of school life. Unless a child has a medical condition that prevents participation, every student must be actively engaged in fitness routines every day.
Schools have a moral and social responsibility to reinforce healthy habits. Nutrition, exercise, and wellness education shouldn’t be treated as add-ons—they must be embedded in the very ethos of our education system. Only then can we truly prepare our children to thrive, both in body and mind.
Q: When hepatitis is transmitted from mother to child during birth, what are the recommended medical interventions and follow-up care protocols to ensure the child’s well-being?
A: The first step in managing paediatric hepatitis is identifying the type of virus the baby has acquired—typically Hepatitis B or C, though A and E are also possible. In most cases involving vertical transmission, Hepatitis B is the primary concern.
If a baby contracts Hepatitis B from the mother, immediate action is critical. The newborn must receive the first dose of the Hepatitis B vaccine within hours of birth, followed by the complete vaccination schedule. This protocol is well established and widely known.
However, if the mother’s viral load is high—meaning her infection is severe—the newborn should also receive Hepatitis B immunoglobulin (HBIG) in addition to the vaccine. HBIG provides immediate passive immunity and significantly reduces the risk of infection. Fortunately, this is available in most tertiary-care hospitals and urban medical centers. But in rural or under-resourced settings, where HBIG access may be limited, ensuring timely vaccination becomes even more crucial.
Hepatitis C presents a different scenario. It rarely affects infants during early infancy in a clinically significant way. However, accurate diagnosis requires caution. We should not screen for Hepatitis C before 18 months of age. Before this age, maternal antibodies—transferred during pregnancy—can lead to false positives without indicating actual infection.
Instead, screen the child at 18 months. If the result is positive, initiate regular follow-up. Thankfully, effective treatment options for Hepatitis C are now available and can be safely administered after the child turns three.
In both cases, timely screening, vaccination, and follow-up remain the cornerstones of effective paediatric hepatitis management. Early intervention can prevent lifelong complications and ensure the child grows up healthy and hepatitis-free.





1 Comment
I always look forward to your posts. Keep it coming!
Comments are closed.